Sedation Training
Introduction to Procedural Sedation Training
#sedation training basics
Author:
Talmage Egan
Jul 29, 2022
Back to blog
I first dived into the topic of sedation training some 20 years ago. As a young physician in an academic medical center, I was tasked by the Department of Anesthesiology Chair to take on the leadership of the Sedation Committee. My charge was to elevate the quality and safety of the sedation in the facility, primarily by promulgating best practices and improving training.
In this role, I discovered the wild and wooly world of sedation practice, particularly as it relates to training. At our facility, we had numerous groups of doctors and nurses practicing procedural sedation at a diverse array of locations, including the emergency room, radiology scanner rooms, procedural suites, endoscopy suites, and clinic exam rooms, among others. I learned that our practitioners were using over 15 different sedation records. Our monitoring practices were quite dissimilar. Most of all, the sedation training that our practitioners could point to as the foundation of their practice (and the basis of their privileges) was highly variable.
Keep in mind that these healthcare professionals were dedicated doctors and nurses. Many of them had considerable experience in performing procedural sedation. But the considerable variability in sedation techniques, practice patterns, and sedation training was concerning.
Gaining Advanced Sedation Knowledge with Improved Training
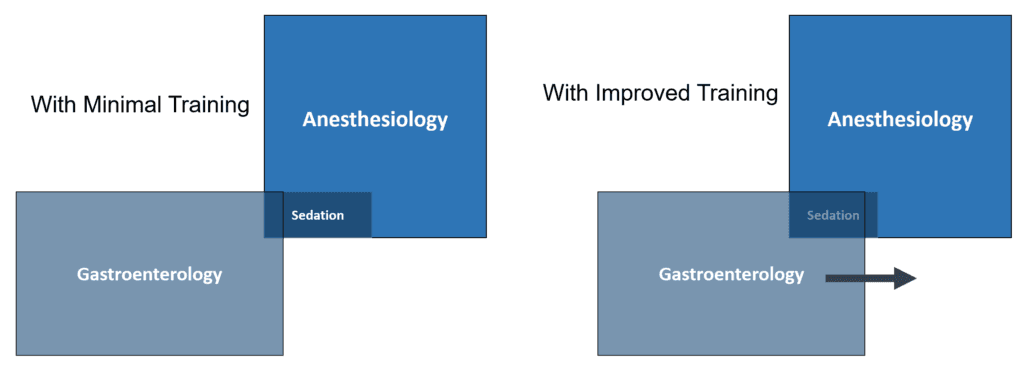
When considered as a Venn diagram, advanced sedation knowledge and skill can be considered a core competency of anesthesiology practice, although it constitutes a relatively small part of the overall field. Similarly, sedation practice should also be reckoned a core competency of medical proceduralists who sedate patients to facilitate certain medical procedures (gastroenterologists who perform endoscopy). The goal of improved sedation training is to increase the overlap of the sedation core competency between the anesthesiologist and the gastroenterologist (or another proceduralist) as illustrated in the simple Venn diagram below.
An important point to emphasize is that sedation training is not resuscitation training. Resuscitation training, such as Advanced Cardiac Life Support (ACLS), as advocated by the American Heart Association, is certainly an important set of knowledge and skill for sedation practitioners to hold. But ACLS is not sedation training. ACLS is focused on the resuscitation of patients who have suffered from cardiopulmonary arrest. This knowledge and skill are applicable only when sedation has gone badly. Sedation training is focused not on resuscitation but rather on elements of sedation practice aimed at improving the quality and safety of sedation so that ACLS skills are less likely to be necessary.
What Sedation Training Curriculum Should Include
There is a general agreement on what sedation training should include. Many professional societies have produced consensus statements outlining a rational curriculum, including anesthesiology, emergency medicine, and gastroenterology professional organizations. Pre-procedure preparation, patient selection, airway assessment and management, sedation pharmacology, clinical monitoring, “rescue” techniques, and post-procedure care comprise some of the critical parts of a rational sedation training curriculum.
Along these lines, the United States Food and Drug Administration (FDA) has recently pronounced in the labeling of a sedation-related device (i.e., The Sedasys System) that sedation practitioners should undergo structured, pragmatic training aimed at:
identifying a high-risk patient
differentiating deep sedation from moderate sedation
assessing the patient for responsiveness, airway adequacy, ventilation, oxygenation, and circulation
monitoring effectively (including capnography)
rescuing a patient from deeper-than-intended sedation
titrating sedatives and analgesics based on pharmacologic characteristics
Pressing Problem of Sedation Training and the Solution to Improve It
The main barrier to implementing such training is that, until recently, there has not been a widely available, standardized, professional society endorsed sedation training curriculum. Experts in various sedation-related fields acknowledge that most sedation training is done “on the job” without a rigorously outlined curriculum and assessment of competency. Most trainees in procedural sedation-related specialties do not receive formal didactic instruction regarding sedation.
So, I learned early on in my role as the sedation committee chair that a primary unmet need in the world of sedation practice was a widely available, standardized training process that could be used as the basis for credentialing and privileging doctors and nurses to perform procedural sedation. The main goal of such training is, of course, to improve the quality and safety of the patient experience. A secondary goal is to provide medical facilities with a basis for credentialing and privileging sedation practitioners. Improvement of the risk management aspects of sedation practice is another reasonable expectation of more advanced training.
It was in this overall milieu that I determined to focus some scholarly and creative energy on this unmet need in sedation training. Thus, the idea of Safe Sedation Training (SST) was born some years ago in collaboration with colleagues at the University of Utah. I am a founder and equity interest holder in the company that markets SST (conflict alert and disclosure!).
The Concept of the SST Program
The Safe Sedation Training program was developed with National Institutes of Health-SBIR support and is endorsed by the American Society of Anesthesiologists (it is their recommended sedation training). The training was also approved by the FDA as appropriate training for certain sedation settings (e.g., Computer Assisted Personalized Sedation systems — CAPS systems). The target audience is nurses and doctors who are not anesthesia professionals by training.
In brief summary, SST is:
a screen-based simulation, distance-learning approach;
grounded in professional society guidelines;
modular, self-paced learning (requiring about 4 hours);
a “Virtual Preceptorship” that includes 3 learning areas for each module (i.e., conference room, simulation center, and sedation suite);
a CME bearing educational experience;
accompanied by a high fidelity simulation training option (i.e., SSTsim) for centers that desire it.
The “Virtual Preceptorship” is perhaps the most innovative concept incorporated into the SST training. For each of the 9 modules, learners visit three different learning areas as depicted below:
The Virtual Conference Room. Concepts are introduced in brief “mini-lectures.”
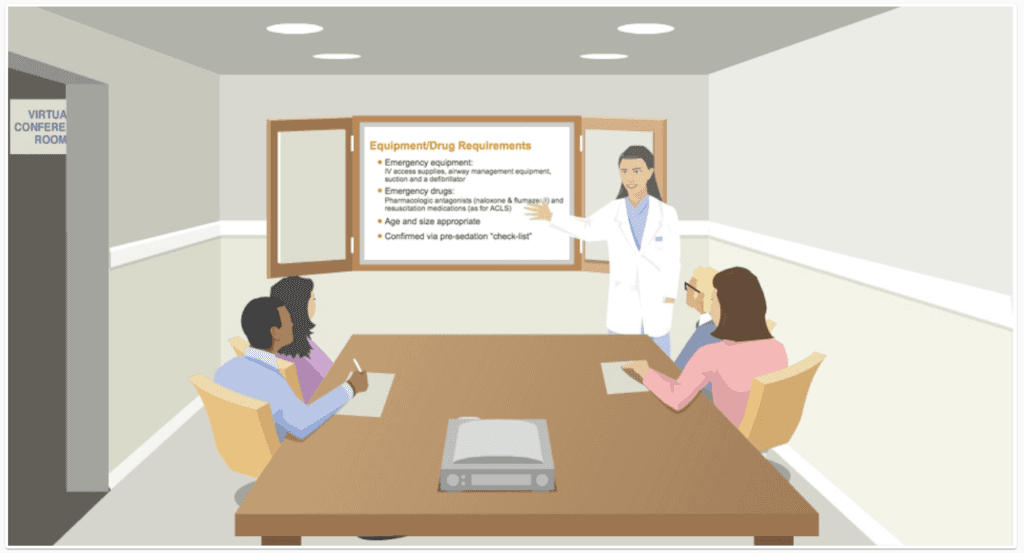
The Virtual Simulation Center. Concepts are reinforced through “workshop” demonstrations.
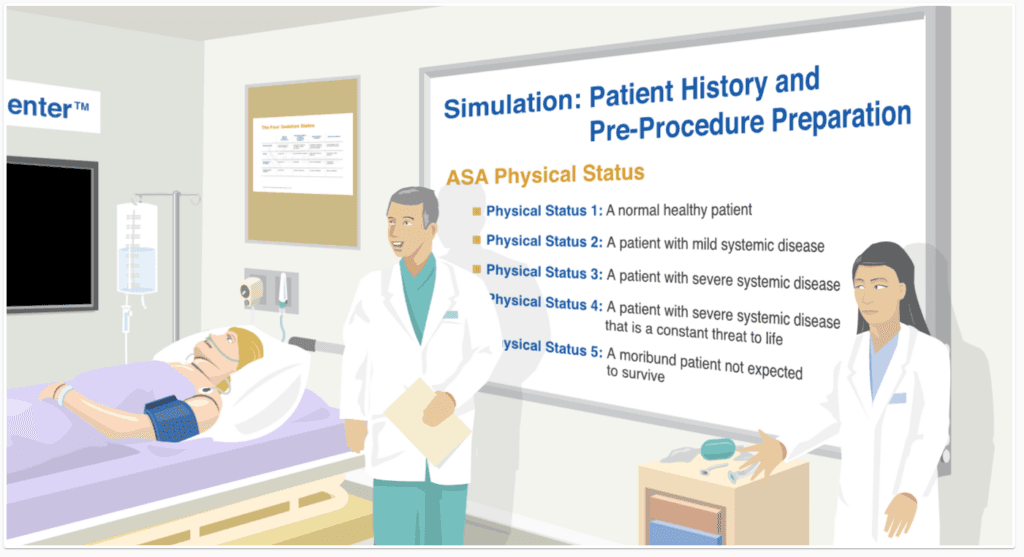
The Virtual Sedation Suite. Concepts are integrated and applied.
The training has now been completed by nearly 16,000 learners and is a common means of sedation credentialing and privileging at many hospitals and clinics in the USA and around the world.
If you would like more information, please visit the SST website.
About the author

Dr. Egan is a professor and chair of the Department of Anesthesiology at the University of Utah School of Medicine. He's a graduate of the University of Utah, and his post-graduate training took place in Utah and at Stanford University. The experience gained from the fellowship training in clinical pharmacology at Stanford, intensive physician executive training at the Harvard School of Public Health, and his sabbatical as a visiting scientist at the Imperial College in London helped Dr. Egan launch SST. Dr. Egan has contributed his expertise to sedation practice over the past 35 years. He published multiple research publications, mostly in the area of anesthetic pharmacology. Dr. Egan's clinical practice and research work have made him one of the leading experts on sedation in the world.