Sedation Training
Sedation Pitfalls: Knowing the Difference Between RESCUE and RESUSCITATION
#sedation
Author:
Ken Johnson
Dec 27, 2022
Back to blog

Introduction
Every sedation practitioner has tales of woe when things go sideways. An apneic patient becomes difficult to ventilate and turns blue, or a patient turns unresponsive with profound bradycardia. After managing one of these challenging situations, a moment of reflection may lead one to consider: was I ready? Was this within my scope of practice? Am I appropriately trained? Will this happen again?
Personalizing sedatives to keep patients comfortable during a painful procedure while maintaining their vital signs stable is a CHALLENGE. It is inevitable that sedation practitioners are not able to always get it right. On rare occasions, it can lead to a near miss and substantial unpleasantness.
So, what does it take to be ready for such events? It’s useful to explore this through the lens of two terms: RESCUE and RESUSCITATION. They require different skills and expertise. Do I have these skills? Do I know the difference?
Review of the Sedation States
The sedation continuum is a useful way to describe levels of sedation. They include minimal, moderate, deep sedation, and general anesthesia. Deep sedation and general anesthesia are inherently more hazardous than minimal or moderate sedation. We discuss the details of sedation states in this blog post.
Knowing how to detect the switch from moderate to deep sedation is especially important. This is the point when patients transition from being able to respond to a prompt to breathe to being unresponsive to such prompts. It is a marker of an increased likelihood of partial or complete airway obstruction, ventilatory depression, or hemodynamic instability. Sedation practitioners must be not only able to detect deeper-than-intended sedation but also be adept at initiating rescue maneuvers.
Rescue Defined
Rescue is defined as interventions needed to correct the consequences of deeper-than-intended sedation. It may include maneuvers even when the patient remains responsive. A qualified rescuer has skills in basic airway management and essential life support techniques and recognizes that continuing a procedure at a deeper level of sedation than intended is problematic.
Rescue is a process meant to head off emergency conditions that require more advanced resuscitative maneuvers. Rescue maneuvers are typically performed by a member of the sedation team; they are anticipated but uncommon.
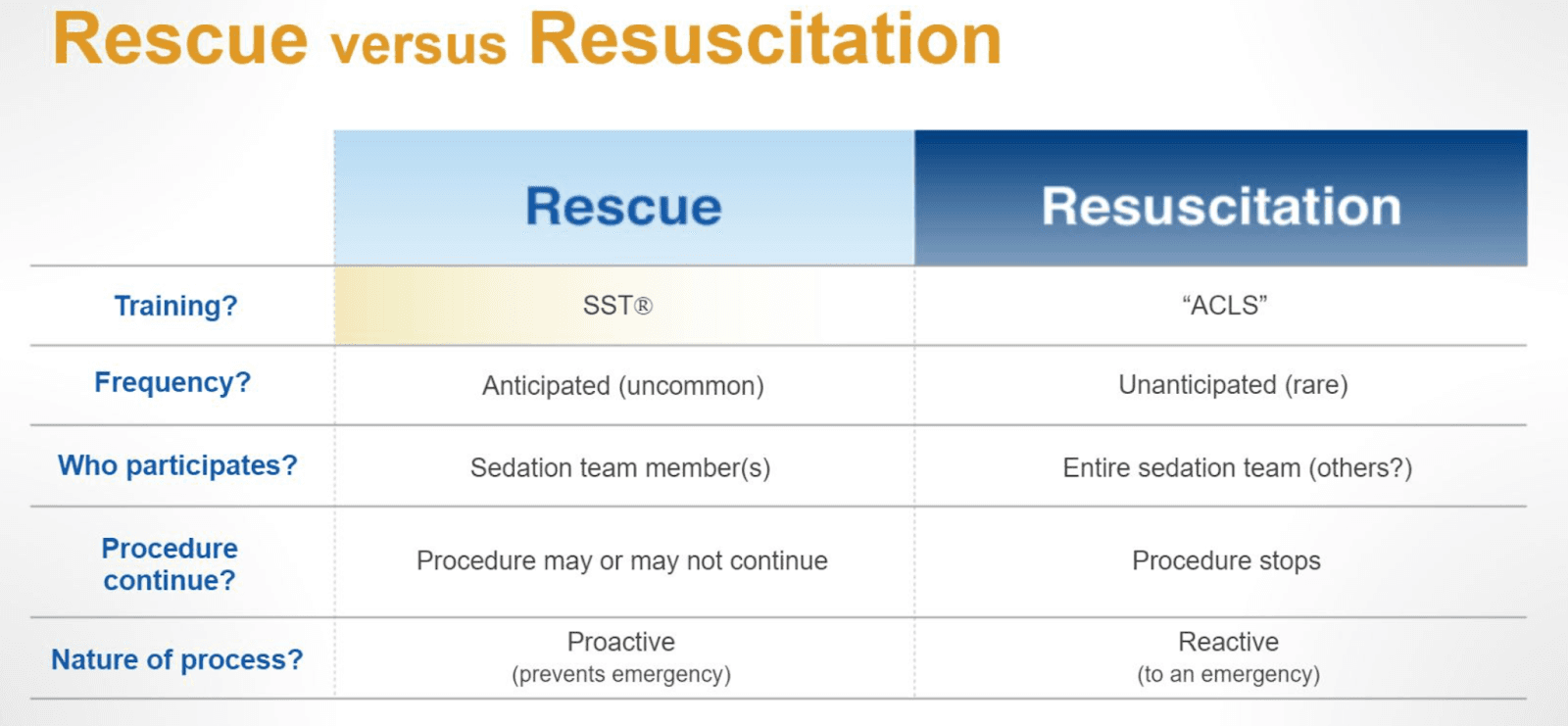
Rescue Versus Resuscitation
If rescue measures fail, ACLS-guided resuscitation may be needed. It should be performed by individuals with advanced life support skills, including starting an IV, knowing how to use a defibrillator, and advanced airway skills to provide effective manual ventilation, placing a supraglottic airway (a laryngeal mask airway (LMA) or tracheal intubation). Resuscitation is needed in an emergency and requires that a procedure be halted immediately. Although these events are rare, if such a person is not a member of the sedation team, the team should have a practitioner with resuscitative skills readily available. This may include utilizing a rapid response team or arranging for a practitioner with this skill set available with a 5-minute response time. To put this time into perspective, brain injury occurs within 4 minutes of brain anoxia.
Let’s summarize the differences between the concepts of rescue and resuscitation during procedural sedation.
When assessing the need for rescue, a useful approach is RAVOC®. This acronym stands for Responsiveness, Airway, Ventilation, Oxygenation, and Circulation and presents a systematic approach to identifying adverse effects of sedation. It is like the ABCs of ACLS. Check out our Safe Sedation Training courses to learn about RAVOC and how to use it effectively during sedation procedures.
The Self-Rescue Concept
Preserving the patient’s responsiveness enables a patient to “self-rescue,” with the provider prompting when airway obstruction or hypoventilation begins to occur. Because the patient is responsive to command, they may be able to self-correct their physiologic issue. Prompting to take a deep breath with or without tactile stimuli is an important rescue tool. Once responsiveness is lost, the patient cannot contribute to their own rescue, and more skilled rescue maneuvers may be required, such as opening an obstructed airway, bag and mask ventilation, and administration of reversal agents. At this level of sedation, it is important to consider whether it is safe to proceed with the procedure. We discuss self-rescue techniques in detail in our Safe Sedation Training courses.
Conclusion
To summarize, rescue maneuvers are basic measures to return a patient to the intended level of sedation. They can include prompting the patient to breathe with tactile or painful stimuli and supporting other vital functions as guided by the RAVOC assessment. When rescue fails, there should be a quick move to halt the procedure, stop sedative administration, call for help, and prepare for resuscitation.
About the author

Dr. Johnson is a Berkeley undergrad with a degree in engineering. His graduate education included a medical degree and a Master of Science in bioengineering from Tulane University. He then received a postgraduate degree in Anesthesiology from the University of Utah. Dr Johnson is the Anesthesiology Chair at the University of Arizona and is the former director of the University of Utah Anesthesiology Center for Patient Simulation for 21 years. He is also an oral board examiner for the American Board of Anesthesiology. Dr. Johnson contributed to the integration of Safe Sedation Training with high-fidelity patient simulation activities and has significantly contributed to SST's scientific foundation.